
The Latest and greatest treatments for IBD: What to believe
What’s the best IBD medicine for me? Confusion on television and in your inbox....
See moresign up for our newsletter
Subscribe
About 20 to 30% of Crohnies (those with Crohn's disease) will develop a painful tunnel from their intestine to the skin around their bottom, known as a perianal fistulas. In fact, as many as 8 to 13% of Crohnies will even have these fistulas when they first come to the doctor.
What is a perianal fistula?
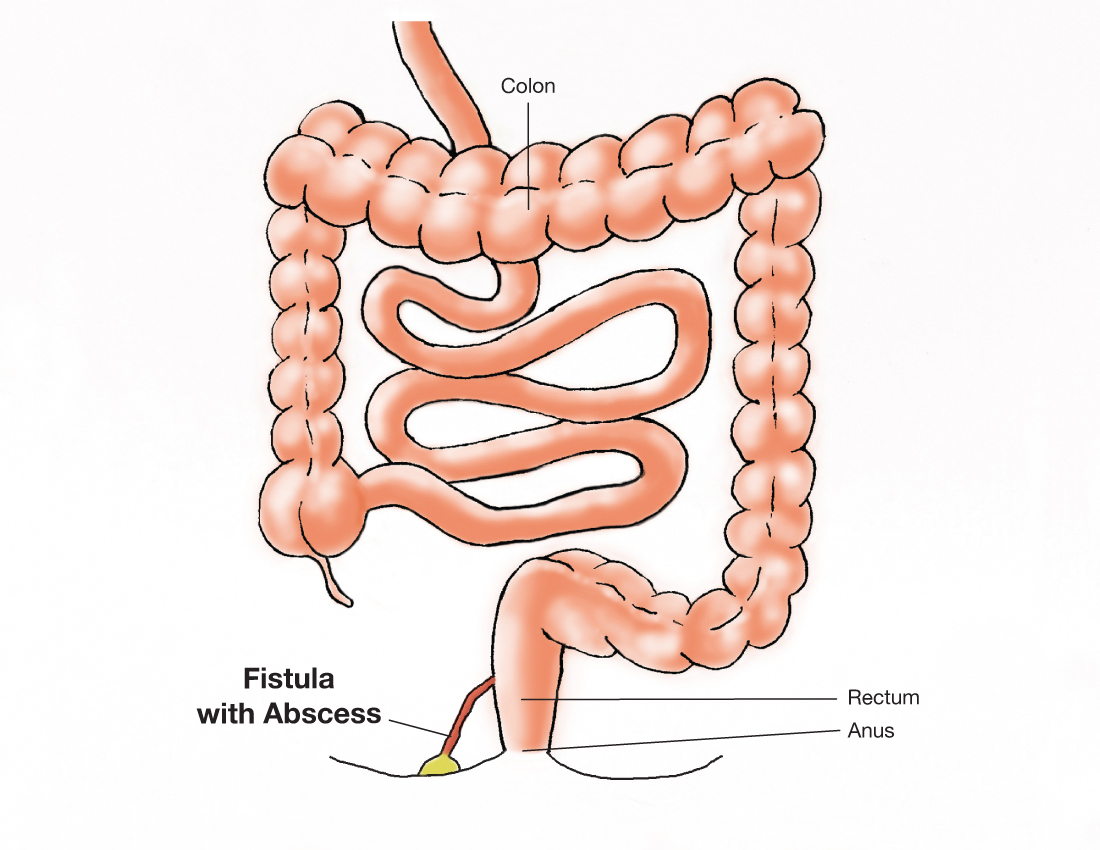
A fistula is the medical term for a tunnel that develops, going from one place to another. Perianal means "around the anus" (the outside part of the rectum–so it's called a perirectal fistula sometimes. In the case of Crohn's disease, that tunnel starts from the intestine, usually from the rectum. And while most times, the tract ends up near the anus, a tract can rarely go towards a woman's vagina or a man's testicles.
The symptoms
There's often a great deal of pain and swelling when the fistula starts to burrow and break through to the skin. Blood and infected debris, known as pus, often comes through the tunnel. At times, an infection builds up inside (an abscess) along with the fistula. That makes the area tender, so that some Crohnies are unable to even sit down.
How's a perianal fistula diagnosed?
A doctors' examination will usually discover a fistula if it's already formed and draining. But if the tract isn't fully formed, MRIs are sometimes needed to find the fistula and to help determine the best way to treat it.
MREs (a MRI or Magnetic Resonance Imaging with contrast added to outline the intestine–making it an enterography) is often used to detect and better understand a person's Crohn's disease. But that can miss a small fistula that's developing unless a regular MRI of the rectal area is added. The combination is much more effective–and has shown undetected fistulas in 12 % of Crohnies who weren't suspected of having them. This testing combination represents a massive breakthrough. Physicians can find the tracts before they become a problem and manage them so that the condition does not worsen.
Treating a fistula
Antibiotics are often used in the beginning to clear up the infection, when that's possible, but then one of the <<biologics>> and sometimes a <<thiopurine>> are often used with good success.
When the medications aren't working by themselves, surgery may be needed. Depending on the location and how severe a fistula is, a seton (a small surgical string) is threaded through the fistula and left in place to help the infection drain, or the outside may be capped off to see if the fistula can close. An abscess may also need to be drained, if one is there. An MRI can be used to tell how the healing is progressing and whether something else may have to be done.
Predictors of Relapse
Unfortunately, fistulas come back (relapse) in about 20%-30% of patients within the first year, even with the best of care. One study found there was no difference in the relapse rates between those who use two different <<anti-TNF>> biologics <<infliximab>> or <<adalimumab>>. But those who stopped their medicine after the fistula healed had a fistula return 3.5 times more often than those who remained on their medicine. So, taking an anti-TNF often works to heal perianal fistulas, but stopping that therapy after the fistulas disappear could give someone a higher chance of a fistula returning.
It's also important to note that disease location, <<Crohn's classification>> and previous surgery all play a role in predicting whether a fistula will return. There's an increased chance of another fistula if someone has:
While this helps us understand how to treat fistulas and prevent their return, more research is needed to completely understand why they start and how to prevent them in the first place.
Additional Reading
Brochard C, Landemaine A, L'Heritier AM, et al. Anal Fistulas in Severe Perineal Crohn's Disease: Mri Assessment in the Determination of Long-Term Healing Rates. Inflamm Bowel Dis. 2018;24(7):1612-1618. doi:10.1093/ibd/izy055
Kim PH, Park SH, Jin K, et al. Supplementary Anal Imaging by Magnetic Resonance Enterography in Patients with Crohn's Disease Not Suspected of Having Perianal Fistulas. Clin Gastroenterol Hepatol. 2020;18(2):415-423.e4. doi:10.1016/j.cgh.2019.07.038
Malian A, Rivière P, Bouchard D, et al. Predictors of Perianal Fistula Relapse in Crohn's Disease. Inflamm Bowel Dis. 2020;26(6):926-931. doi:10.1093/ibd/izz200
This article, as well as all others, was reviewed and edited by a member of our Medical Advisory Board.
Subscribe Be the first to know


